As state legislatures convene for their 2022 sessions, addressing the public health and economic impacts of COVID-19 will remain front and center. In addition, many states will continue to decide how to allocate federal funding from the American Rescue Plan. Common themes in financing recovery efforts include sustaining new or renewed partnerships with community stakeholders to fortify emergency response capabilities and build community resilience, addressing long-standing and exacerbated health inequities, and increasing access to higher quality care. Hospitals play an important role in our communities as anchor institutions and are key stakeholders in these recovery themes. Many hospitals and health systems also have benefitted financially from federal funding in the past year and can be engaged as key partners in sustainable, value-driven approaches. Accordingly, as states move forward with COVID-19 recovery, they can consider hospital community benefit investments as another source for community health improvement.
To learn more about hospital community benefit policy, visit NASHP’s resource page.
NASHP developed a tool to help states assess hospital community benefit spending on health equity.
Hospital Community Benefit Policy
In exchange for their tax-exempt status, non-profit hospitals are required to report community benefit expenditures and investments in community health. The federal requirements for non-profit, tax-exempt hospitals have changed over time to reflect the shifting perspective of what factors influence health and what role hospitals should play in community health improvement.
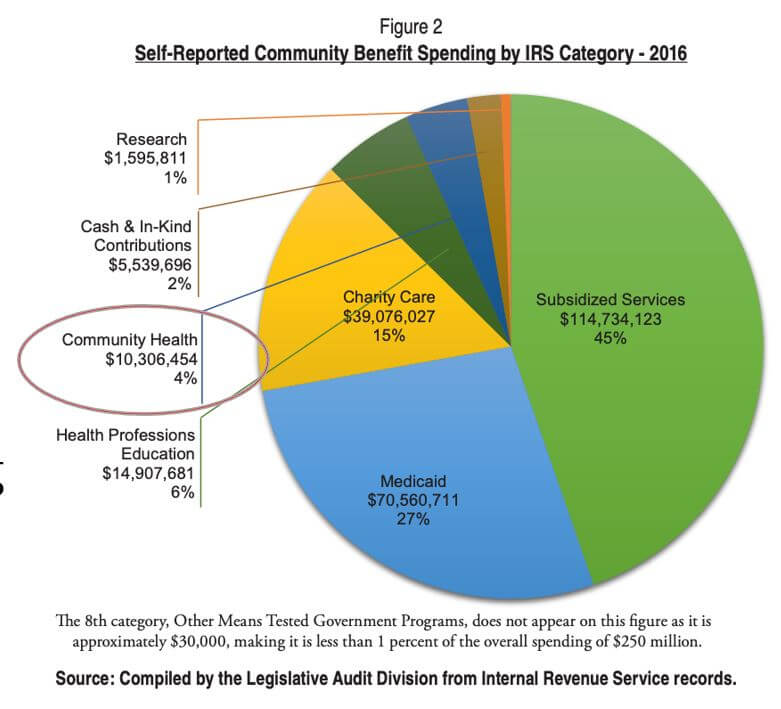
In 2009, the Internal Revenue Service (IRS) updated the Form 990 Schedule H to require more detailed reporting of community benefit expenditures across seven different categoriesincluding charity care, unreimbursed costs from means-tested government programs, community health spending, research, and others. The Affordable Care Act added requirements that non-profit hospitals 1) complete community health needs assessments (CHNAs) every three years to identify the most pressing community health priorities, and 2) create detailed implementation strategies explaining how the identified needs will be addressed.
Despite these changes, there remain significant opportunities for hospital investments to align with community-identified needs and gaps in federal oversight of hospitals’ community benefit programs. While there is congressional interest in pursuing additional clarity at the federal level about what activities constitute sufficient community benefit provision, state legislatures also are addressing enhanced transparency in and accountability of hospital community benefit programs.
2021 Community Benefit Legislation
In 2021, a number of states were interested in overseeing how hospitals implement federal community benefit requirements. Eight states introduced community benefit bills and four states enacted this legislation. Enacted legislation includes:
California Assembly Bill No. 1204. Under existing law, private non-profit hospitals must adopt a community benefit plan that “describes the activities the hospital has undertaken to address identified community needs within its mission and financial capacity, including health care services rendered to vulnerable populations,” and must submit the plan to the Department of Health Care Access and Information (HCAI) no later than 150 days after the hospital’s fiscal year ends.
This new law signed by Governor Newsom further defines vulnerable populations to include:
- Racial and ethnic groups experiencing disparate health outcomes, including Black/African American, American Indian, Alaska Native, Asian Indian, Cambodian, Chinese, Filipino, Hmong, Japanese, Korean, Laotian, Vietnamese, Native Hawaiian, Guamanian or Chamorro, Samoan, or other nonwhite racial groups, as well as individuals of Hispanic/Latino origin, including Mexicans, Mexican Americans, Chicanos, Salvadorans, Guatemalans, Cubans, and Puerto Ricans.
- Socially disadvantaged groups, including all of the following:
- The unhoused;
- Communities with inadequate access to clean air and safe drinking water, as defined by an environmental California Healthy Places Index score of 50 percent or lower;
- People with disabilities;
- People identifying as lesbian, gay, bisexual, transgender, or queer; and
- Individuals with limited English proficiency.
AB 1204 also requires hospitals and hospital systems to annually submit an equity report starting in 2025 that includes an “analysis of health status and access to care disparities for patients on the basis of age, sex, race, ethnicity, language, disability status, sexual orientation, gender identity, and payor.” The report must include a plan to address disparities identified by the data with measurable objectives and timeframes. The bill allows HCAI to impose a fine up to $5,000 if a hospital fails to adopt, update, or submit an equity report. The bill requires HCAI to set up a Health Care Equity Measures Advisory Committee that will assist with recommendations and analysis of the equity reports.
Florida HB 7061. In 2020, HB 7079 was passed requiring a hospital seeking a county property tax exemption to submit its IRS Form 990, Schedule H to the state. It also limited a hospital’s county tax exemption to the value of the net community benefit expense it provided according to its schedule H. HB 7061 removes these requirements and tax limitations.
Illinois SB 1840. This law aims to advance health equity by lowering hospital costs for low-income and uninsured residents and increasing transparency of community benefit plan information. Currently in Illinois, non-profit hospitals annually file their community benefit plan with the Attorney General. The law makes several changes to community benefit reporting requirements including:
- Requiring non-profit hospital community benefit plans to describe “activities the hospital is undertaking to address health equity, reduce health disparities, and improve community health.”
- Health systems must report charity care spending and financial assistance application data separately for each individual hospital.
- Adding definitions for charity care and bad debt to include:
- Charity care: includes the actual cost of services provided based upon the total cost to charge ratio derived from a non-profit hospital’s most recently filed Medicare Cost Report Worksheet C and not based upon the charges for the services. “Charity care” does not include bad debt.
- Bad debt: the current period charge for actual or expected doubtful accounting resulting from the extension of credit.
- Requires hospitals to post their hospital community benefit plan on their website. The plan must include charity care costs, total net patient revenue, total community benefits spending, and information on financial assistance applications, including submission and demographic (i.e., race, ethnicity, sex, and language) data.
Washington HB 1272. In Washington, non-profit hospitals must make their CHNAs available to the public and make their implementation strategy publicly available within one year of submitting their CHNA. This law aims to make hospital operations more transparent, and it includes a requirement that non-profit hospitals identify community health improvement activities that cost $5,000 or more and that designated critical access or sole community hospitals report information for the 10 highest cost community health improvement activities. These activities are reported through an addendum to their CHNA starting July 1, 2022. The addendum must include:
- The type of activity;
- The method in which the activity was delivered;
- How the activity relates to an identified community need in the community health needs assessment;
- The target population for the activity and strategies to reach the target population;
- The identified outcome metrics;
- The cost to the hospital to provide the activity;
- The methodology used to calculate the hospital’s costs;
- The number of people served by the activity; and
- Which organization administered the activity, whether it was the hospital or another organization.
Additionally, the law requires that hospitals report demographic data about the people involved with the CHNA process and requires that hospitals include the following groups:
- Community organizations that provide community health improvement services;
- Communities impacted by health inequities;
- Health care workers;
- Hospitals; and
- The governor’s interagency coordinating council on health disparities.
Community Benefit Policy in 2022 and Beyond
The legislation in 2021, both enacted and introduced, shows the broad range of policy levers available to states to address hospital community benefit policy. As states look towards public health and economic recovery, hospital community benefit investments can be considered as a source of funding to improve community health.
States can go beyond the current community benefit federal requirements to ensure non-profit investment in communities through a variety of levers including:
Conducting state audits to determine the impact of community benefit spending;
- The Montana Legislative Audit Division calculated the total amount of community benefit spending by non-profit hospitals in Montana, and used the Robert Wood Johnson County Health Rankings to evaluate the relationship between such spending and community health improvement.
Requiring non-profit hospitals to submit detailed financial information to a state entity;
- The Maryland Health Services Cost Review Commission requires hospitals to report, among other information, the cost of each community benefit initiative and provide a financial reporting template to capture detailed information.
Setting a minimum spending amount on community benefit.
- The Oregon Health Authority sets a spending floor in collaboration with hospitals every two years based on an identified methodology.
To learn more, read the National Academy for State Health Policy’s (NASHP) report, Resources to Help States Maximize their Hospitals’ Community Benefit Investments. To join NASHP’s work on community benefit or for more information contact Elinor Higgins.
Support for this work was provided by the Robert Wood Johnson Foundation. The views expressed here do not necessarily reflect the views of the foundation.