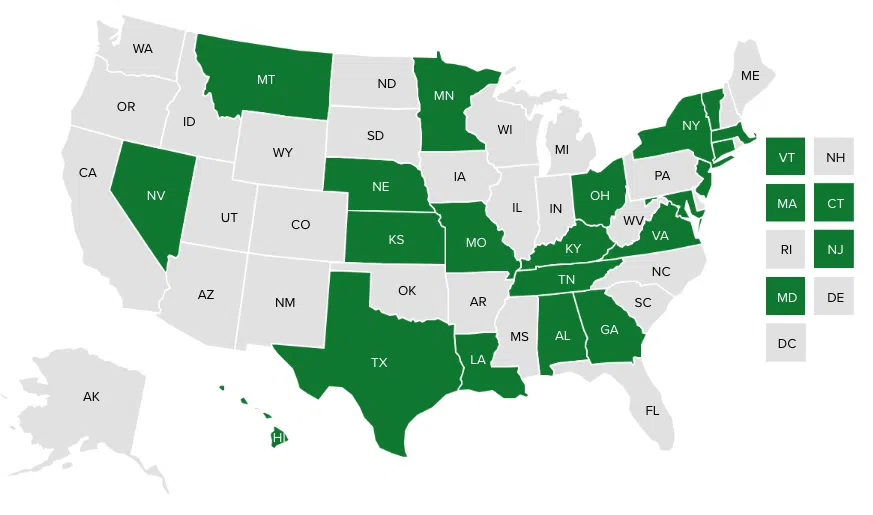
More than a dozen states are developing accountable health models to improve population health and control costs by addressing community needs, such as transportation, recreation, and housing. These entities’ mission — to build healthy communities through cross-sector partnerships — is supported by innovative and evolving governance structures. This NASHP chart and a companion blog highlight how states are structuring these entities to keep them accountable and reflective of their communities.
![]() Print this chart.
Print this chart.
California
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| California Accountable Communities for Health Initiative (CACHI) | “An accountable communities for health (ACH) must establish a sound governance structure that ensures effective decision-making; accountability to the community; representation of stakeholders’ interests; proper fiduciary, fiscal, and social responsibilities; and control over funding and staff.” (ACH Legal & Practical Recommendations, p. 4) An ACH should have a set of rules (bylaws or agreement) to hold stakeholders accountable to their obligations, defined fiduciary duties for the Governing Body, established controls over activities and finances, and a conflict of interest policy and procedure.” (p. 4) |
The ACH collaborative must include: “-Health plans, hospitals, private providers or medical groups and community clinics serving the geographic area. -Government health and human services agency/public health department -Grassroots, community and social services organizations that include authentic and diverse representation of residents, particularly from underserved communities.” “It is desirable that every ACH include broad representation of several of the following types of entities: -County and/or city government leadership, including elected officials -Behavioral health providers – Housing agencies -Food systems -Employers and other business representatives -Labor organizations -Faith-based organizations -Schools and educational institutions -Parks and recreational organizations and agencies -Transportation and land use planning agencies -Dental providers -Local advocacy, grassroots organizations or policy-focused organizations.”(RFP, p. 7) |
CACHI’s Year 1 request for proposals awarded points for, “Meaningful resident engagement and a process for ongoing engagement throughout the funding period.” (RFP, p. 14) | Recommended key milestone: “By the end of Year 1: Develop a governance plan that includes the following: -A list of community sectors to be represented on the Governing Body of the Wellness Fund. -An outline of key components of bylaws to establish the number of directors, meetings, voting procedures, a community investment committee, and conflict of interest and anti-nepotism policies. -A document outlining how accountability to the community will be achieved and maintained (e.g., by reserving board and committee slots for community residents and providing annual reports on activities and spending).” (ACH Legal & Practical Recommendations, p. 35-36) |
Colorado
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| Colorado Regional Accountable Entities | “The contractor shall have a governing body responsible for oversight of the Contractor’s activities in relation to this Contract.” (RFP 5.3.5) |
“The contractor shall select members of the governing body in such a way as to minimize any potential or perceived conflicts of interest.” (5.3.5.1) | “The regional accountable entities (RAE) will develop mechanisms to engage community partners within the RAE’s region for population health and nonmedical community services.” (3.3.10) The RAE will “promote physical and behavioral health ….[and] the population’s health and functioning, coordinate care across disparate providers, interface with long-term services and supports providers, and collaborate with social, educational, justice, recreational and housing agencies to foster healthy communities ….” (3.3.3) |
The contractor shall publicly list information, including, but not limited to, the names of the members of the governing body and their affiliations, on the contractor’s governing body on the contractor’s website.” (RFP, 5.3.6) | “The program will focus on greater coordination with the Colorado Departments of Human Services, Public Health and Environment, Education, and Corrections, as well as initiatives such as Comprehensive Primary Care Plus (CPC+), State Innovation Model (SIM), Hospital Transformation Program, and the Colorado Opportunity Project. The RAE will play key regional roles in these initiatives as they are well aligned with the Accountable Care Collaborative’s goals.” (3.3.11) |
Connecticut
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| Connecticut Health Enhancement Communities (HECs) | “Health Enhancement Communities (HEC) will have a defined structure, with a formal governance structure and community organizing groups. The formal governance structure will have clearly defined decision-making roles, authorities, and processes. The community organizing groups will have ownership and decision-making authority over the things that matter most to them and will lead the identification and implementation of interventions in their communities.” HEC Design Principles (See p. 52-54 of HEC model design draft proposal, Oct. 22, 2018, for chart of other governance requirements.) |
“-In addition to community organizing groups, HECs will need to identify multiple methods for gaining meaningful involvement, including in decision-making, as HECs form and operate -HECs will need to include multiple community organizations that directly address root causes of poor health in their communities.” (HEC model design draft proposal p. 52) |
“Given their unique and essential perspectives and insights about their communities, HECs’ success depends on the ongoing involvement of community members and community members making decisions about things that matter most to them. In addition to community members being involved in HEC formation and operation, the HEC structure should also support community organizers and locally owned and directed community organizing groups within communities….” (HEC model design draft proposal p. 9-10) | Minimum governance structure elements required by the state and determined by HECs: “-Partnership agreements -Bylaws -Backbone organization -Formal contracts for services.” (HEC model design draft proposal p. 52-53) |
State Innovation Model |
Delaware
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| Delaware Healthy Neighborhoods | Neighborhood task forces: “Create and propose data driven, evidence-based initiatives, request funds…measure outcomes… engage in quality improvement. Local councils “serve as a ‘board’ of the Healthy Neighborhood (e.g. decision making about resource allocation)… [and] approve Task Forces’ requests for resources.” (HMA, Healthy Neighborhoods Model, Dec. 2017, p. 7) The role of the fiscal agent is to: -“Distribute funding to entities implementing Task Force Initiatives (once ‘readiness process’ has been completed) -Collect data/outcomes from each Task Force related to funded initiatives and utilize this practice of continuous analysis as a tool for ongoing learning -Focus on sustainability of the SIM Grant funding (e.g., establishing and managing a community trust) -Serve as a ‘Backbone Organization’ across all Local Councils.”(HMA, p. 4) |
Local neighborhood task forces contain: “-Local community stakeholders and leaders that are focused on a priority area -Two co-chairs.” Local councils are made up of: “-At least one representative from each task force -Local leaders with expertise in priority areas -Cross-sector entities and organizations recruited via the Social Network Analysis to ensure representation of all critical entities -Delivery systems as well as community-based organizations -Community advocates from neighborhoods -Community stakeholders.” (HMA, p. 7) “Voting procedures are established in the bylaws of the Local Council.” (HMA p. 18)Local councils are advised by a statewide consortium with: “-Local council co-chairs -Statewide leaders focused on user-friendly community-level data -Statewide leaders focused on sustainability of healthy neighborhoods -Statewide leaders focused on policy -Advocacy organizations from neighborhoods -The statewide fiscal agent.” (HMA p. 8) |
“Readiness assessment will assess: -Did the task force use data about community needs to develop the initiative? -Did the task force include representatives from diverse entities who weighed in on the creation of the plan? -Similarly, do you have community buy-in?” (p. HMA 15-16) |
State Innovation Model |
Massachusetts
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| Massachusetts Accountable Care Organizations (ACOs) | Massachusetts Health Policy Commission (HPC)’s ACO Certification Program assessment criteria includes a “Patient-centered, accountable governance structure.” (ACO Policy Brief, April 2018, p. 3) |
“The ACO provides for meaningful participation in the composition and control of the Governing Body for its participants or their representatives.” ACOs must attest that “ACO Participants have at least 75% control of the Governing Body (Proposed 2019 ACO Certification Standards, p. 7). – [ACOs must have] “at least one patient or consumer advocate within the governance structure.” (Proposed 2019 ACO Certification Standards, p. 7-8) |
“The ACO governance structure is designed to serve the needs of its patient population, including by having … a patient and family advisory committee.” (Proposed 2019 ACO Certification Standards, p. 7-8) | The HPC requires ACOs to submit an “Organizational chart(s) of the Governance Structure(s) of the Applicant (and Component ACOs as applicable), including Governing Body, executive committees, and executive management, and indicating the location of a patient or consumer representative role within each Governance Structure.” (Proposed 2019 ACO Certification Standards, p. 5-6) ACOs are required to submit a Full Participation Plan that includes “The providers and organizations with which the ACO is partnering or plans to partner, the governance structure … [and] a population and community needs assessment.” (p. 14) |
MassHealth Medicaid Section 1115 Demonstration |
| “The ACO Governing Body regularly assesses the access to and quality of care provided by the ACO, in measure domains of access, efficiency, process, outcomes, patient safety, and patient experiences of care, for the ACO overall and for key subpopulations (i.e. medically or socially high needs individuals, vulnerable populations), including measuring any racial or ethnic disparities in care.” (Proposed 2019 ACO Certification Standards, p. 8) | ACOs are required to submit a Full Participation Plan that includes “The providers and organizations with which the ACO is partnering or plans to partner, the governance structure … [and] a population and community needs assessment.” (DSRIP protocol, p. 14) |
Michigan
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| Michigan Community Health Innovation Regions (CHIRs) | “Each of the five regions is supported by a backbone organization that serves as a fiduciary and acts as a neutral convener for the CHIR’s governing body.” “CHIR partners are organized by a neutral backbone organization that [serves as a fiduciary and] facilitates the development and implementation of key strategies, creating the necessary capacity to sustain progress on stated objectives. CHIR steering committees provide a clear leadership structure and promote shared accountability among partners for aligning their resources to address priority community health needs.” (SIM, “About CHIRS”) |
“CHIR governance facilitates effective collaboration of providers, health plans, community based organizations and individuals to pursue community‐centered solutions to upstream factors of poor health outcomes and health disparities.” (NASHP slides, Aug. 2018) | State Innovation Model |
Minnesota
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| Minnesota Accountable Communities for Health (ACHs) | “The lead organization is responsible for convening a multi-sectoral governing body with representation from partner organizations and the community. ACH projects are exploring and testing a variety of governance approaches such as charters, formal business agreements between partners and use of technical subcommittees …. ACH leadership team structure and makeup differs across ACHs. Some ACHs created an entirely new governance structure while others use existing committees, task forces, or advisory bodies (such as Statewide Health Improvement Program – SHIP – committees) to organize their work.” (ACH: Perspectives on Grant Projects and Future Considerations, Oct. 2016, p. 12). “Besides leadership and governance, the ACH must have a ‘backbone’ or lead organization to serve as convener and integrator.” (p. 35) |
“Each ACH has a lead organization (e.g., private foundation, non-profit social service agency, local public health agency or health care system) that serves as fiscal agent and resources manager. The lead organization is responsible for convening a multi-sectoral governing body with representation from partner organizations and the community.” (ACH: Perspectives on Grant Projects and Future Considerations, p. 12) “All health plans and systems serving the population should participate in the ACH. Local public health must be an active partner, and local political leaders, government officials and other leaders should be invited to participate. Most importantly, the governing body should ensure that persons experiencing health disparities are represented in ACH partnerships, mission and vision.” (ACH: Perspectives on Grant Projects and Future Considerations, p. 35) |
“Each ACH grant project features … community-led leadership.” (Minnesota Accountable Communities for Health) | Required components of each ACH grant project are: “-Community-led leadership -Care coordination between multi-sectoral partners -Population-based prevention -Measurement and evaluation -Partnership with an Accountable Care Organization -Participation in an ACH learning community -Sustainability planning -Health equity focus.” (Minnesota Accountable Communities for Health) |
New York
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| New York Performing Provider Systems (PPSs) | “The Performing Provider System will need to demonstrate that it has a governance strategy that ensures that participating providers work together as a “system” and not as a series of loosely aligned providers nominally committed to the same goal.” (DSRIP Program Funding and Mechanics Protocol, p. 14) | “Please explain how the selected members provide sufficient representation with respect to all of the providers and community organizations included within the PPS network. Please outline where coalition partners have been included in the organizational structure, and the PPS strategy to contract with community based organizations.” (DSRIP PPS Organizational Application, p. 35) |
“Describe how the PPS governing body will engage stakeholders on key and critical topics pertaining to the PPS over the life of the DSRIP program.” (DSRIP PPS Organizational Application, p. 34-36) | Medicaid Section 1115 Demonstration Delivery System Reform Incentive Payment program | |
| “Describe the decision making/voting process that will be implemented and adhered to by the governing team. Explain how conflicts and/or issues will be resolved by the governing team.” (DSRIP PPS Organizational Application, p. 35.) | State Health Innovation Plan (through the State Innovation Model) | ||||
| State Health Improvement Plan (the Prevention Agenda). |
Oregon
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| Oregon Coordinated Care Organizations (CCOs) | “Coordinated care organizations may be local, community-based organizations or statewide organizations with community-based participation in governance or any combination of the two.” (2017 ORS 414.625) “Each coordinated care organization’s governing body establishes standards for publicizing the activities of the coordinated care organization and the organization’s community advisory councils, as necessary, to keep the community informed.” (ORS 414.625) |
“Each coordinated care organization has a governing body of which a majority of the members are persons that share in the financial risk of the organization and that includes: (a) A representative of a dental care organization selected by the coordinated care organization; (b) The major components of the health care delivery system; (c) At least two health care providers in active practice, including: (i) A physician licensed under ORS chapter 677 or a nurse practitioner certified under ORS 678.375 (Nurse practitioners), whose area of practice is primary care; and (ii) A mental health or chemical dependency treatment provider; (d) At least two members from the community at large, to ensure that the organization’s decision-making is consistent with the values of the members and the community; and (e) At least one member of the community advisory council.” (2017 ORS 414.625) |
Required to serve on the governing body are: “At least two members from the community at large, to ensure that the organization’s decision-making is consistent with the values of the members and the community; and At least one member of the community advisory council.” (2017 ORS 414.625)Community advisory councils: “A coordinated care organization must have a community advisory council to ensure that the health care needs of the consumers and the community are being addressed. The council must: (a) Include representatives of the community and of each county government served by the coordinated care organization, but consumer representatives must constitute a majority of the membership; and (b) Have its membership selected by a committee composed of equal numbers of county representatives from each county served by the coordinated care organization and members of the governing body of the coordinated care organization.” (2017 ORS 414.627) |
Medicaid Section 1115 Demonstration |
Rhode Island
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| Rhode Island Accountable Entities (AEs) | “The intent of these requirements include: 1) To ensure multi-disciplinary providers are actively engaged in a shared enterprise and have a stake in both financial opportunities and decision-making of the organization; (2) to ensure that assets and resources intended to support RI Medicaid are appropriately allocated, protected, and retained in Rhode Island; (3) to ensure that the mission and goals of the new entity align with the goals of EOHHS and the needs of the Medicaid population; (4) to ensure a structured means of accountability to the population served.” (AE Certification Standards, 2017, p. 16) |
“There shall be an established means for shared governance that provides all AE Partner Providers with an appropriate, meaningful proportionate control over the AE’s decision-making process.” (AE Roadmap, April 2017, p. 42) “Board or Governing Committee Membership. The majority of voting members of the Board or the Governing Committee shall be provider representatives from participating Partner or Affiliate provider organizations, provided that at least three members shall be LTSS providers and one member shall be a behavioral health provider. Minimal representation requirements for each population certified to serve -Children: pediatric representative member of Consumer Advisory Committee, community-based organization (CBO) provider of age-appropriate supports -Adults: representative member of Consumer Advisory Committee, CBO provider of age-appropriate social supports (AE Certification Standards, 2017, p. 45) |
Draft certification standards include a requirement for AEs to have a “Community Advisory Committee consisting of at least ten persons who are attributed Medicaid beneficiaries who are representative of the populations served by the AE.” (AE Roadmap, 2.1.8) | Medicaid Section 1115 Demonstration | |
| State Innovation Model (SIM) |
Vermont
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| Vermont Accountable Communities for Health (ACHs) | “An accountable community for health is managed through a governance structure that articulates the process for decision-making and outlines the roles and responsibilities of the integrator organization, the steering committee (or other decision-making body), and other collaborative structures or partners.” From Vermont Accountable Communities for Health Peer Learning Lab Report, March 2017 |
“The governance structure should include a diverse representation of stakeholders, including decision-makers, experts, community members, and leaders from the variety of community organizations that impact health in the region.” (Vermont ACH Peer Learning Lab Report, p. 18). | “The ACH Peer Learning Lab sought to build on this framework and test model implementation while increasing community capacity and readiness across the nine Core Elements of the ACH model.” (Vermont ACH Peer Learning Lab Report, p. 6 ) |
Governance is one of the nine core elements of the ACH model. (Vermont ACH Peer Learning Lab Report, p. 18) |
Washington
| State | Description, Goals, and Functions of Governing Body | Representation in Governing Body | Community Engagement | Governance Accountability, Incentives, or Milestones | Connection to Other State Initiatives |
| Washington Accountable Communities of Health (ACHs) | Accountable communities of health must: -Maintain a governance structure that includes balanced cross-sector collaboration and decision-making, including the necessary documented procedures and agreements, e.g. bylaws and a memorandum of understanding. -Ensure that no one sector or organization can control decision-making. -Revisit the process at least annually to determine effectiveness considering the regional landscape and specific governance structure.” (State Innovation Model Contractual Guidelines for Accountable Communities of Health, P. 5)“Minimum expectation: ACHs must develop and maintain a communications framework to keep partners informed and involved in between meetings and events.”(State Innovation Model Contractual Guidelines for Accountable Communities of Health, p. 8). |
“Washington’s tribes and urban Indian health organizations (UIHOs) are among the partners ACHs should reach out to for participation in ACH activities, including governance and decision making… Tribal governments are not stakeholders. The state maintains relations with the tribes on a government-to-government basis.” (State Innovation Model Contractual Guidelines for Accountable Communities of Health, p. 7) | “ACHs require governance structures tailored by community leaders to most effectively implement the goals of Healthier Washington at the local level.” (State Innovation Model Contractual Guidelines for Accountable Communities of Health, p. 5). “Because of the unique regional demographics, existing resources, and potential initiatives already under way, the specific community engagement strategies will not be prescribed by the state.” (State Innovation Model Contractual Guidelines for Accountable Communities of Health, p. 8). |
“Minimum expectation: ACHs must implement a cascading engagement approach tailored to the local environment that brings the voice of consumers and individual community members to ACH development and decision making, in addition to the balanced multi-sector decision making structure.” (State Innovation Model Contractual Guidelines for Accountable Communities of Health, p. 8) “ACHs are strongly encouraged, under the SIM contract, to maintain open public governing body meetings.” (State Innovation Model Contractual Guidelines for Accountable Communities of Health, p. 8) |
State Innovation Model |