This project is a partnership between NASHP and The Health Reentry Project (HARP).
Introduction
States are taking advantage of new opportunities to cover certain health services under Medicaid for youth and adults exiting incarceration. Successfully implementing these new policies designed to improve health outcomes requires systems and data bridges across historically siloed systems. States are prioritizing efforts to share data across state agencies and with local partners (such as correctional facilities and community-based providers) to determine program eligibility, support continuity of clinical care and supports, facilitate payment, and evaluate programs.
The Allegheny County, Pennsylvania, integrated data warehouse fosters effective data sharing and systems integration to support individuals’ transitions from incarceration to the community. This brief focuses specifically on Allegheny County’s strategies around clinical information sharing and may inform state-level systems and data integration work and/or serve as a model to identify community-level data sharing that could be scaled or disseminated.
Allegheny County Integrated Data Warehouse
For more than 20 years, the Allegheny County Department of Human Services (DHS) in Pennsylvania has maintained an integrated data warehouse that enables person-specific information sharing, drawing data from a variety of partners, including the county jail.
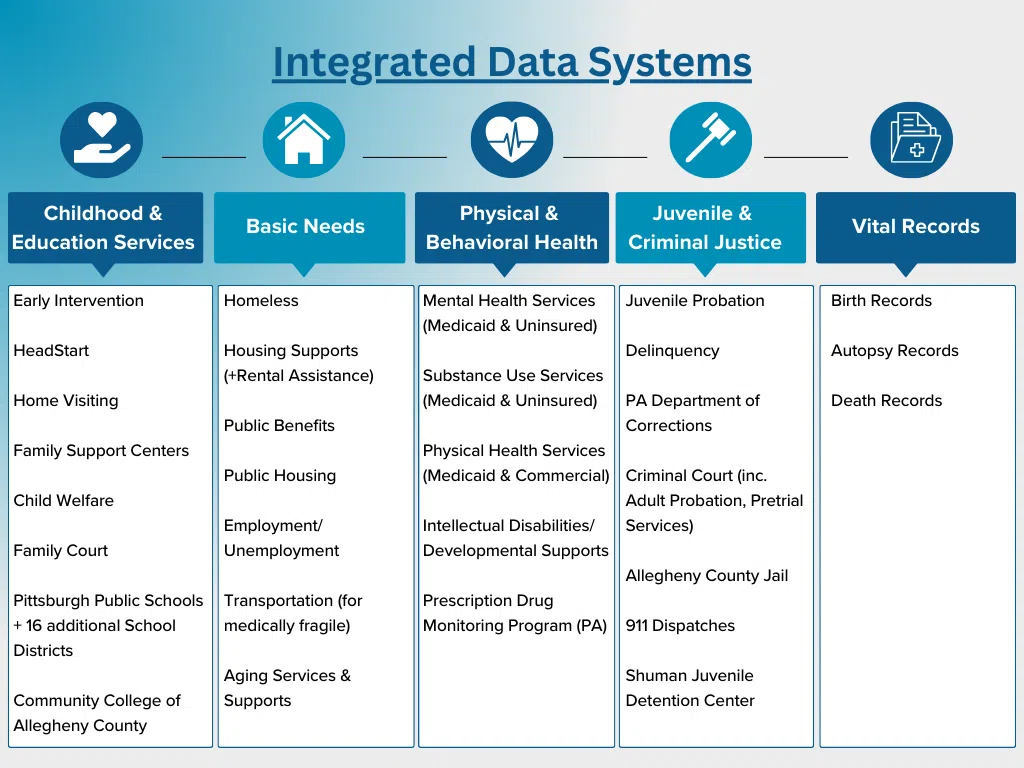
The data warehouse was initially funded through pooled local foundation funding and is currently maintained by DHS, representing less than 1 percent of DHS’s total budget. This integrated data warehouse enables understanding of individual-level service activity across programmatic areas and services administered by DHS – such as child welfare, mental health, drug and alcohol, homelessness, aging, and others – as well as activity provided by other sources, such as Allegheny County Jail, Public Housing Authorities, and the Pennsylvania Department of Human Services (see Figure 1 for the full list of data sources).
Notably, it draws from both public and commercial health insurance plans. The county has agreements with commercial health plans to enable a more universal representation of the county’s residents. DHS employees and its contracted provider network may access data in the warehouse, and clients may access their own information using custom applications. To facilitate communication, each individual’s service record includes contact information for their providers.
Figure 1: Integrated Data Systems
Communicating Data Sharing Principles
Allegheny County DHS has taken several actions to support its contracted providers and partners in safely sharing information. The county developed a data sharing framework and clearly communicated state, federal, and county level rules around data sharing to providers, including providing examples of official data sharing agreements to support implementation of data sharing initiatives.
DHS leadership developed a data sharing philosophy that recognizes the importance of data sharing for coordinated care and communicates an approach for sharing data and obtaining consent to ensure compliance with federal and state confidentiality laws. DHS articulated this philosophy in a memo for contracted service providers.
As an entity with oversight and coordination responsibilities, DHS states their overarching goal is to “achieve an appropriate and respectful balance that ensures quality care and services through collaboration and coordination, supported by appropriate use and sharing of client data.” The memo clarifies that Allegheny County, of which DHS is a part, defines itself as a hybrid covered entity under the Health Insurance Portability and Accountability Act (HIPAA) for all program areas and business operations, meaning that the health department and nursing facilities are covered entities, but not the entire county.
To facilitate data sharing, DHS has created a template data sharing agreement (DSA) and Memoranda of Understanding (MOU) – see an example MOU between DHS and Pittsburgh Public Schools). These agreements define each partner’s responsibilities and requirements. In data agreements, DHS remains flexible around definitions of data elements rather than listing out every specific element. This gives them flexibility to request additional data if needed to support the evolution of their coordination and oversight efforts.
Sharing Mental Health and Substance Use Information for People in Allegheny County Jail
Allegheny County’s integrated data warehouse is central to coordinated care transitions for individuals in the county jail. Some services in the jail are provided by the Allegheny Health Network medical system physicians and other providers, who have access to the jail electronic health record (EHR). Additionally, the jail employs nurses, care coordinators, and recovery coordinators on their health care staff who have access to the jail’s EHR. The list below and Figure 2 illustrate how data are shared to coordinate care for individuals with mental health needs and substance use disorder (SUD) during their stay and upon release.
Pre-arraignment: Upon entry into the jail, a social worker uses the data warehouse to view an individual’s behavioral health history. This information can be used, with consent, to share information on a pre-arraignment diversion plan document with the public defender and arraignment judge to determine if it would be appropriate for the individual to be released under supervision and connected to treatment in the community at the time of first appearance (arraignment). This information helps the social worker understand what services the individual might need to access if they remain at the jail. HIPAA-protected information is stored in the jail’s EHR and only shared with, and accessible to, health care staff. Health care staff may share limited information with corrections officers directly supervising the individual only if it is needed to keep the individuals safe, such as an individuals on suicide watch or with a seizure disorder.
Booking:
- At the time of booking, all individuals are screened for eligibility to participate in Justice Related Services (JRS), or service coordination for justice-involved individuals. In addition to service coordination, JRS can provide release planning and transitional supports. Once a JRS release plan is approved by the judge, DHS utilizes an internal dashboard to identify individuals waiting for release and monitor their length of stay. Individuals found not competent to stand trial and in need of restoration services are supported by the Mobile Competency Restoration and Support Team, a new initiative in Allegheny County. The County is creating a dashboard to track and measure outcomes for these services as well.
- The data warehouse generates a daily report showing all the individuals who have been booked into the jail the previous day who received publicly funded mental health services within the prior six months. This report is shared with behavioral health care staff in the jail to inform their care while at the jail. It is also shared with the DHS Office of Behavioral Health’s managed care provider, who notifies providers when their patient enters the jail. This prevents individuals who were receiving services prior to incarceration from having to complete the intake process a second time to resume services when they reenter the community.
- For individuals who self-report use of medications for the treatment of opioid use disorder (MOUD), jail medical staff use a program called Surescripts, an electronic prescription platform that interfaces with the Pennsylvania Prescription Drug Monitoring Program to verify previous MOUD and connect the individual to MOUD in the jail. If a person reports they are taking methadone for the treatment of opioid use disorder, the jail refers them to the methadone provider in the jail, who must obtain the individual’s consent before coordinating with the community treatment provider. The jail is also able to initiate methadone or buprenorphine treatment for individuals.
Reentry to community:
- JRS, or the Mobile Competency team, provides support throughout the transition from jail to community for many individuals with mental health challenges. If another community treatment team is involved with the individual, jail healthcare staff may facilitate a reconnection to the provider to support reintegration and continuity of care.
- The jail employs an SUD case manager who connects individuals receiving MOUD to community providers upon reentry. Additionally, individuals receiving MOUD are eligible to participate in a Reentry Peer services program that ensures a warm handoff to community treatment providers while also providing general reentry supports. Many individuals are referred through the jail electronic health record (EHR) to the River Clinic, a post-incarceration clinic, and Unity Recovery, which provides reentry peer support services. The River Clinic receives a daily report of referrals as well as a daily report of releases via EHR notification. Data from the prescription drug monitoring program helps to ensure individuals can continue to access the medications they need upon reentry. Unity Recovery has view-only access to see the individual’s records in the EHR and receives a daily report of jail releases.
Leveraging aggregate-level, deidentified data from the warehouse, the county created a dashboard for researchers and the general public highlighting populations who are receiving MOUD in Allegheny County Jail, as well as associated outcomes before and after their release.
Figure 2: Sharing Mental Health and Substance Use Info for People Arrested and Brought to the Allegheny County Jail
Considerations for States
States working to expand their capacity to support transitions from incarceration may use this example to inform their own data sharing systems or partner with locals to create a similar system. Key best practices for states from Allegheny County include:
- Identify a clear use case to drive the work, rather than tackling the whole system at once. The Allegheny County example is robust and has taken many years to develop. Allegheny County officials encourage states and locals aiming to replicate their work to identify a clear use case and advance manageable, concrete changes that can build over time that they want to achieve. This should include articulating a state’s ultimate goal, what information should be shared, and who the information should be shared with – while ensuring compliance with federal and state laws.
- Obtain and leverage buy-in from a leadership champion. Look to leaderships’ defined priorities and requirements the state must comply with – such as the CAA of 2023 requirements for youths returning from incarceration – and how data sharing is necessary to meet those goals. For example, this may include the Governor’s office, the Secretary of Corrections, and/or the Secretary of Health and Human Services.
- Assess what data, systems, process, and sharing are currently in place.
States can conduct a scan of data, systems, processes, and sharing that may already be available for use or that could be scaled or disseminated – working with regional, county, or local partners to identify existing infrastructure, community partnerships, and data systems. Note that a key element of systems and data integration includes mapping by whom and how correctional health services are provided – by a vendor, correctional staff, community providers, or hybrid versions thereof. It is also important for states to take stock of existing resources and understand capacity-building needs. For instance, whether correctional facilities already have access to EHRs and how they differ, to community information exchanges, and/or to a data warehouse available in their community or at the state level. Working with local partners to understand the state role in building that capacity is key to enhance and not disrupt effective strategies in the interest of standardization.
- Begin with relationships and data governance; complicated technological solutions are not necessary to start.
Relationships and data governance, such as data sharing agreements and MOUs, are necessary to get data flowing and protect privacy and confidentiality. In some cases, data sharing agreements can take months to years to get in place so it’s best to start early. On the other hand, complicated technology solutions are often a barrier for states due to their cost, state procurement processes, and the level of expertise and information needed to build systems. Luckily, they are not necessary to get started. Secure exchanges of information that are less technologically advanced can still be used to share the needed information while states pursue more technologically advanced or automated approaches.
Policy, administrative, data, legal, and technology leads are likely to have different goals and constraints about what is possible. For example, Allegheny County found having the leads of each perspective involved in decision-making conversations streamlined the process and reduced back-and-forth on decisions.
- Bring policy, administrative, data, legal, and technology leads into the same room for decision-making conversations.
Policy, administrative, data, legal, and technology leads are likely to have different goals and constraints about what is possible. For example, Allegheny County found having the leads of each perspective involved in decision-making conversations streamlined the process and reduced back-and-forth on decisions.
- Consider seeking outside counsel that specializes in privacy laws.
Government agency internal counsel may not have specialized experience in privacy law. Outside counsel with expertise in privacy laws, particularly those with a behavioral health, health care, and criminal justice focus, may provide input that creates a framework for improved data sharing and reduce unnecessary barriers.
Conclusion
NASHP, in partnership with The Health and Reentry Project (HARP), supports states with a Learning and Action Network and the State Reentry Learning Collaborative, a multi-state technical assistance opportunity for states actively implementing Medicaid reentry waivers. NASHP will continue to support states in building the data infrastructure to strengthen intersections across health and corrections and support individuals’ health and social needs upon reentry from incarceration.
Additional Resources
- Allegheny Specific Resources:
- State Health and Value Strategies and Manatt Health: Information-Sharing Considerations for Implementing the Consolidated Appropriations Act’s Requirements for Justice-Involved Youth
- Network for Public Health Law: Equitable and Effective Data Sharing to Support Healthy Transitions for Youth During Reentry
- Actionable Intelligence for Social Policy: “Finding a Way Forward: How to Create a Strong Legal Framework for Data Integration.”
- CRISP DC: Consent Tool for data protected by 42 CFR Part 2, which is integrated with their health information exchange and updated to align with the February 2024 final rule relating to 42 CFR Part 2.
- Additional local examples of integrated data sharing systems include:


